Radioactive decay is inherently probabilistic. It’s not possible point at a particular unstable atom and predict when it will decay. Further, some types of unstable atoms have more than one path for decay; it’s also not possible to predict the path of a single atom.
The behavior of large numbers of atoms, however, is statistical, and we can say some things about their collective radioactive decay: half of the atoms present will decay within a time called the half-life, and the fractions of atoms that take the various paths of decay are predictable.
When probabilistic physics is combined with the uncertainties and unknowns of biology, prediction becomes much more difficult. Ingested radioactive materials are excreted from the body in times also measured by half-lives. Whether radiation kills a cell or alters its DNA is probabilistic. Whether that altered DNA leads to cancer is probabilistic. And we don’t know the probabilities of those events, although we can derive some overall numbers from epidemiology.
What we know about radiation effects on the human body comes largely from epidemiological studies of the survivors of the Hiroshima and Nagasaki atom bombings in 1945 who were exposed to very high levels of radiation. Those effects are expressed in probable numbers of cancer deaths per number of people exposed. The effects of low levels of radiation, those that most people encounter, require studying extremely large numbers of people. Such studies are prohibitively expensive, so few have been done, and those effects have been extrapolated down from the higher exposures. There is a great deal of controversy surrounding this approach. It is more likely to overestimate probable numbers of cancers than to underestimate them.
The limits set on radiation exposure, therefore, represent a judgement about the acceptable increase in cancers in a population. Background levels of radiation and other contributors to cancer vary from place to place, so additional radiation at sea level may still be less than natural exposure at higher altitudes, making this judgement still more complicated.
The International Commission on Radiological Protection (ICRP) provides the basis from which national radiation protection standards are developed, but nations and subnational bodies decide what level of protection is desirable.
For example, the US Environmental Protection Agency prefers a risk of 1 in a million that an individual will develop cancer in a lifetime as a goal for environmental remediation, but the US Nuclear Regulatory Commission assesses the risks differently. A report by the US General Accounting Office (now General Accountability Office, GAO) from the year 2000 provides some helpful general discussion on radiation standards in addition to its discussion of the differences between agencies in developing standards for the Yucca Mountain Repository. (At the time the report was written, rem was the commonly-used unit of biological radiation effect. Today, sievert is the unit in use. One sievert equals 100 rem.)
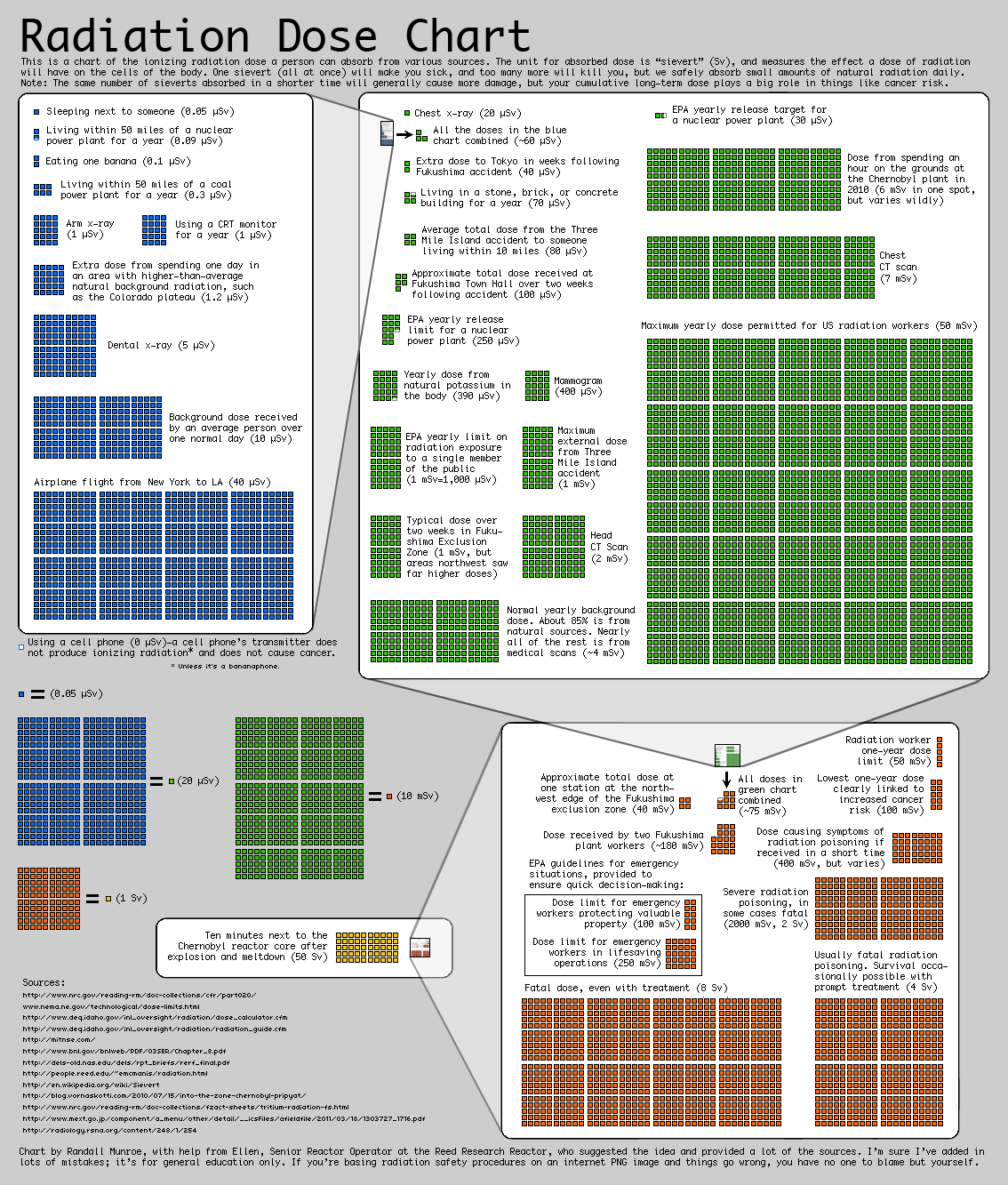
The chart by XKCD gives the EPA yearly limit on radiation exposure to a single member of the public as 1 mSv (green area, about halfway down the left-hand side). It gives the yearly limit for a radiation worker as 50 mSv. The ICRP has issued exposure recommendations for Fukushima that allow up to 20 mSv per year for citizens in the area, “with the long-term goal of reducing reference levels to 1 mSv per year.”
The differences in these levels represent judgements that the risk to the public should be less than the risk assumed by workers who understand that they are raising their risk level. The higher exposure levels represent higher risks of cancer. But they start from a one-in-a-million risk for the general population.
{kind=link}
1 comment:
I really could have used that GAO report about six months ago. Ah, well.
Post a Comment